The duty to inquire begins at initial contact and continues until a tribe provides confirmation of tribal membership status or the court makes a finding that proper and adequate further inquiry has been conducted, and there is no reason to know whether the child is an Indian child.
Note: If known or reason to know exists, a social worker or representative from the tribe should be included in the information gathering and screening process, including the screening decision whenever possible. See BIA list of ICWA designees to support noticing and collaborative assessment.
This contact should not prevent or delay the agency from responding within the required timeframe when indicated.
Reason to know. Information exists at the time of the report that indicates a child in the household is an Indian child, including the following.
- The child, family, or a person having interest in the child provides direct information that the child is an Indian child.
- The residence of the child, the child’s parents, or Indian custodian is on a reservation or in an Alaskan Native village.
- Any participant in a court proceeding, officer of the court, Indian tribe, Indian organization, or agency provides information indicating the child is an Indian child.
- The child gives reason to know that the child is an Indian child.
- The child is or has been a ward of a tribal court.
- The parent or child possesses an identification card indicating membership or citizenship in a tribe.
Reason to believe. Information at the time of the report suggests that either the child or a parent of the child may be eligible for membership in an Indian tribe or may have Indian ancestry. Further inquiry is required.
A social worker or representative from the tribe was successfully contacted and included in the information gathering and screening process. Details of the contact must be documented in CWS/CMS, including which tribe(s) were contacted, a summary of information discussed, and the impact on decision making.
If contact with tribe was attempted but not successful, document efforts within CWS/CMS.
- No child under age 18. The current referral may allege abuse or neglect, but the alleged victim is 18 years of age or older (including nonminor dependents). Do not apply this item if the report concerns the death of the only child(ren) in the household where death is suspected to be related to abuse or neglect, or for nonminor dependents reported to be endangered by caregiver, per WIC 16504 (c).
- Duplicate referral that contains no new information. The report duplicates an existing referral (this is commonly known as a secondary referral). This report does not contain new allegations from an existing referral.
- Referred to another county. A referral has been received for a child who lives in another county. The caller was both referred to that county and provided with contact information, or the county was notified and the referral was recorded in that county. Refer to local protocol for this type of referral.
A dependent or ward in out-of-home care is defined as a child/youth who is under the jurisdiction of the county child welfare or probation department AND is currently placed in a licensed foster home, group home, short-term residential therapeutic program, or residential treatment facility.
If yes: When applying definitions of screening and response priority tools, the definition of “caregiver” should include “a person responsible for the child’s care and welfare (including a licensee, administrator, or employee of any facility licensed to care for children)” in accordance with Cal. Penal Code § 11165.5.
If no: Apply screening and response priority tool definitions using the standard SDM definition of “caregiver.”
Consider age, developmental status, and other child vulnerabilities when assessing referrals for allegations of abuse or neglect.
Physical Abuse (if not automatic 24-hour, go to physical abuse tree)
- Physician reports that the injury type is consistent with non-accidental injuries;
- Injury to a non-ambulatory child with no plausible alternative explanation;
- Explanation for injury does not match injury;
- Injury is in the shape of an object (e.g., loop marks); or
- Credible disclosure by the child to the reporting party or other adult.
Identify the type of non-accidental or suspicious physical injury.
-
Death of a child due to abuse (automatic 24-hour). There was a death of a child in the home; and circumstances are suspicious for abuse, or abuse has been identified as the cause of death in this report or investigation. Select one of the following options.
- Death of only child or all children in home; no other children reported to be in the home.
- Other children reported to be in the home.
- Severe (automatic 24-hour). A severe injury is one that, if left untreated, would cause permanent physical disfigurement, permanent physical disability, or death. Include visible injuries and suspected injuries due to symptoms such as loss of consciousness, altered mental status, inability to use an arm, inability to bear weight, etc.
-
Other injury (exclude very minor issues unless child is under 1 year old)
- Any non-accidental or suspicious injury that is not severe.
- Exclude very minor injuries, defined as those that involve only mild redness or swelling, minor welts/scratches/abrasions, or brief and minor pain. Any non-accidental injury to a child under 1 year old or a child who is non-ambulatory should not be considered very minor.
- Injuries caused to a child during a domestic violence incident.
- “Other” injuries may require assessment/treatment but are not life threatening and are not likely to result in temporary or permanent disability or disfigurement. These may include bruises, welts, or abrasions in areas of the body that do not pose a threat of serious injury or disfigurement (arms, legs, buttocks).
- Shaking or throwing an infant or child under 3 years old.
- Inappropriate physical discipline, such as choking, suffocation, tying child up, locking child in closet/kennel, physical activity exceeding child’s ability to perform, etc.
- Hitting a child with enough force or using objects to strike a child that could cause a significant injury, such as a broken bone, concussion, significant bruising or lacerations, or internal injuries.
- Exposing a child to dangerous weather or environmental hazards (e.g., locking child out of the home, confining child to garage with dangerous fumes/exhaust, dropping child off far from home with no resources to get to a safe place).
- Dangerous behavior toward the child or in immediate proximity of the child, including violence by one or more adult household members occurring while the child is present in ways that the child could be physically injured. Consider combination of child location, type of incident (e.g., pushing, throwing objects, use of a weapon), and child vulnerability.
- Caregiver has made credible threats to cause physical harm to the child that, if carried out, would constitute child abuse, and it is likely that, without intervention, the caregiver will carry out these threats. If threats are clearly for the sole purpose of emotional abuse, select “Caregiver actions have led or are likely to lead to child’s severe anxiety, depression, withdrawal, or aggressive behavior toward self or others” under emotional abuse. If the purpose cannot be discerned, select both this section and the emotional abuse item mentioned above.
Emotional Abuse (go to emotional abuse tree)
- Rejecting and/or degrading the child.
- Isolating and/or victimizing the child by means of cruel, unusual, or excessive methods of discipline.
-
Exposing the child to brutal or intimidating acts or statements, including but not limited to:
- Harm or threatened harm to animals;
- Threats of suicide or harm to family members (including the child);
- Confining the child in places such as closets or animal cages; or
- Consistently scapegoating the child; consistently berating, belittling, blaming, targeting, or shaming the child.
The child has experienced, or is likely to experience, emotional harm related to exposure to domestic violence. The child may exhibit harm through symptoms of depression, significant anxiety or withdrawal, or self-destructive or aggressive behavior from witnessing or intervening in physical altercations, serious verbal threats, coercion, or intimidation by one adult household member against another.
Note: If a child has been injured or is threatened with injury, also select “non-accidental or suspicious injury” or “caregiver action that likely caused or will cause injury” under “Physical Abuse.”
Neglect
- Diagnosed malnutrition (automatic 24-hour). The child has a current diagnosis by a qualified medical professional of severe malnutrition due to inadequate or unbalanced diet, OR a qualified medical professional states that there are indicators of malnutrition but a formal diagnosis has not yet been made.
- Non-organic failure to thrive. The child has a current diagnosis by a qualified medical professional of non-organic failure to thrive, OR a qualified medical professional states that there are indicators of failure to thrive but a formal diagnosis has not yet been made.
-
Child’s health/safety is endangered. The caregiver has willfully not provided adequate clothing, shelter, supervision, care, or medical care AND there is imminent danger of serious illness or injury; or serious illness, serious injury, or death has already occurred. Consider child’s age, behavior, and vulnerability. For example:
- The child’s clothing is so inappropriate for weather that the child suffered hypothermia or frostbite;
- Housing conditions result in lead poisoning, severely exacerbated asthma due to smoke exposure, and/or multiple bites from pest infestations;
- There is methamphetamine production in the home/residence;
- Medical care has not been provided for an acute or chronic condition and, as a result, the child has required or is likely to require hospitalization or surgery; or the condition may worsen to the extent that unnecessary permanent disability, disfigurement, or death results;
- Caregiver is willfully not meeting child’s mental health needs and child has demonstrated suicidal or homicidal behavior/ideation;
- Child is not supervised to the extent that the child has been seriously injured, is at risk of being seriously injured, or avoided serious injury only due to intervention by a third party;
- A young child is left in a motor vehicle during extreme temperature conditions;
- A caregiver behaves recklessly in proximity to child (e.g., driving under the influence with a child in the car, using weapons, etc.); or
- Caregiver is breastfeeding while using dangerous substances (type of substances and/or amount resulted in or is likely to result in serious injury/illness to child).
-
Death of a child due to neglect (automatic 24-hour). There has been a death of a child in the home due to neglect or circumstances that are suspicious for neglect. Select one of the following options.
- Death of only child or all children in home; no other children reported to be in the home.
- Other children reported to be in the home.
Note: General neglect does not include a parent’s economic disadvantage and should be limited to circumstances in which the caregiver willfully or negligently fails to provide care. A child must be at substantial risk of suffering serious physical harm or illness to fall within the definition of general neglect (PC 11165.2, WIC 300(b)(1)(A-D)). This applies to all the following subcategories.
- Inadequate food. The caregiver willfully or negligently failed to provide sufficient food to meet minimal requirements for the child to maintain health and growth. The child experiences unmitigated hunger; lack of food has a negative impact on school performance. Caregiver’s use of food stamps and/or food pantries as sources of food should not be considered failure to provide food.
-
Inadequate clothing/hygiene. The caregiver has willfully or negligently failed to meet the child’s basic needs for clothing and/or hygiene to the extent that the child’s daily activities are negatively impacted and/or the child develops or suffers a worsening medical condition. Examples include but are not limited to:
- Sores, infection, or severe diaper rash;
- Inability to attend school due to persistent or recurring lack of clean clothing; and/or
- Experiencing shame or isolation from peers due to poor hygiene/extreme body odor.
-
Inadequate/hazardous shelter. The residence contains hazards that have led or could lead to injury or illness of the child if not resolved. Examples include but are not limited to:
- Housing that is an acute fire hazard or has been condemned;
- Exposed heaters, gas fumes, or faulty electrical wiring;
- No utilities (e.g., water, electricity, heat source if needed) AND these are necessary based on current conditions and age/developmental status or special needs of the child;
- Pervasive and/or chronic presence of rotting food, human/animal waste, or infestations;
- Presence of poisons, guns, or drugs within reach of child; and/or
- Lack of safe sleeping arrangements for infant/child.
-
Inadequate supervision. Caregiver is present but not attending to the child, or caregiver has made inadequate care arrangements for the child. Injury has occurred due to lack of supervision or been avoided due to third party intervention. Examples include but are not limited to the following:
- Caregiver fell asleep in the apartment/house and young child wandered from the home into the hallway/street.
- Child plays with dangerous objects (e.g., sharp knife, gun, matches).
- Non-mobile infant left in car seat or carrier for extended periods of time.
- Caregiver is unable to care for child due to substance use, mental illness, or developmental disability.
- Caregiver does not protect child in the home from a sibling with violent behavior.
- Inadequate medical/mental health care. Child has a mild to moderate condition, and the caregiver is not seeking or following medical treatment, causing the child’s condition to deteriorate; OR the child has a severe, chronic condition and the caregiver’s care is partial, but important components of the child’s medical needs are unmet.
-
Caregiver absence/abandonment.
- Caregiver is unable to care for the child due to incarceration, hospitalization, or unavoidable absence AND there is no safe adult to care for the child. If the caregiver is incarcerated, hospitalized, or absent and has made a plan of care for the child with a safe adult or is otherwise able to safely mitigate the impact of their absence on the child, this item should not be selected.
- Caregiver has deserted the child with no apparent plans for return. Abandonment may be indicated by quitting jobs, establishing another residence, and taking clothing and other belongings.
- Child is being discharged from a facility and caregiver refuses to accept child back into their home AND has not participated in discharge planning or caregiver cannot be found.
- Caregiver has kicked child out of the home/refuses child entry to the home and has not provided a safe alternative.
- Caregiver left child with family or friends who state an intention to discontinue care and caregiver refuses to accept child back or cannot be located.
- Child is or has been left without an identified caregiver for a period of time inappropriate to the child’s age or developmental status. Consider presence of support systems such as relatives and neighbors and child’s ability to access support systems by phone or access within immediate walking distance.
-
Involving child in criminal activity. The caregiver causes the child to perform or participate in illegal acts that:
- Create danger of serious physical or emotional harm to the child;
- Expose the child to being arrested; or
- Force a child to act against their wishes.
-
Failure to protect.
- Note: Concerns related to domestic violence should be assessed under emotional abuse and physical abuse items. Caregiver knowingly left child in the care of a person known to neglect or abuse children; a person unknown to the caregiver; or a person known to be violent, use alcohol/drugs, or have serious mental health concerns to the extent that their ability to provide care is significantly impaired;
- Caregiver does not intervene despite knowledge (or reasonable expectation that the caregiver should have knowledge) that the child is being harmed (includes physical, sexual, or emotional abuse or neglect) by another person; OR
-
A child has been exploited by a third party, and the person responsible for the child’s care is aware of the exploitation and has not acted protectively. This includes situations where the person responsible for the care of the child has been coerced or is otherwise complacent with exploitation.
Note: Screeners should explore a caregiver’s knowledge and protective actions prior to applying allegations of failure to protect. Circumstances in which a child is trafficked and the caregiver may have acted protectively but was unable to keep the child safe should be assessed under “sexual exploitation: Child/youth is exploited or trafficked by someone other than a caregiver.”- Children and youth aged 17 years old and younger are sexually exploited when they have engaged in, solicited for, or been forced to engage in sexual conduct or performance of sexual acts in return for a benefit, such as money, food, drugs, shelter, clothing, gifts, or other goods, or for financial or some other gain for a third party. The sexual conduct may include any direct sexual contact or performing any acts, sexual or nonsexual, for the sexual gratification of others. These acts constitute sexual exploitation regardless of whether they are live, filmed, or photographed.
-
Prior failed reunification or severe neglect, and new child in household (in-home only). There is credible information that a current caregiver had one or more children for whom there was:
- A failed reunification as a result of child abuse or neglect; OR
- A current caregiver was previously substantiated for severe neglect; AND
- A new child is now living in the home and current conditions exist that create a substantial likelihood that the child will be neglected.
-
Allowing child to use alcohol or other drugs. Caregiver provides (offers or knowingly allows the child to consume) alcohol, illegal drugs, or inappropriate prescription drugs to a child to the extent that it could endanger the child’s physical health or emotional well-being or result in exposure to danger because the child’s thinking and/or behavior are impaired. Consider child’s age and substance type, including the following:
- Providing methamphetamine, heroin, cocaine, or similar drugs to a child of any age.
- Providing enough alcohol to result in intoxication.
- Providing alcohol over time so that the child is developing a dependency.
- Providing medications (includes prescription and over-the-counter) that are not prescribed for the child, for the purpose of altering the child’s behavior or mood.
- Providing glue or other inhalants to a child of any age.
Examples of substance use that should not be included are:
- Use of small amounts of alcohol for religious ceremonies; and
- An older child is permitted to try a small amount of alcohol at a family occasion that did not result in intoxication.
- Prior death of a child due to neglect AND there is a new child of any age in the home (in-home only). There has been a death of a child in the home due to neglect or circumstances are suspicious for neglect prior to the current referral, AND new children are currently in the care of the identified/suspected perpetrator.
-
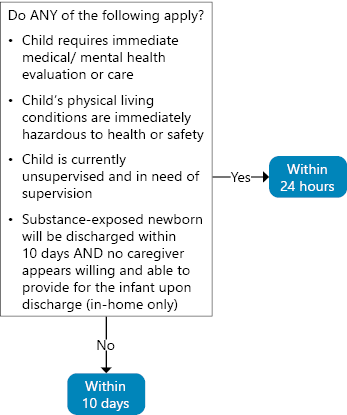
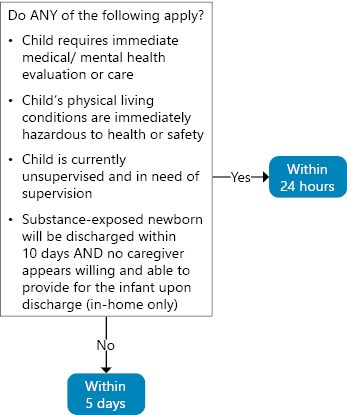
Substance-affected newborn (in-home only). There is an infant born and identified as affected by substance use AND there is indication that the caregiver will be unable to fulfill the basic needs of the infant upon discharge from the hospital.
When assessing caregiver’s ability to provide minimum sufficient level of safe care, consider factors such as willingness to implement a plan of safe care, demonstrations of safe care of other children, plans for safe feeding, and availability of and willingness to use a support network.
Note: California defines an “infant born and identified as affected by substance abuse” as an infant where substance exposure is indicated at birth AND subsequent assessment identifies indicators of risk that may affect the infant’s health and safety. A positive toxicology screen at the time of the delivery of an infant is not in and of itself an indication of neglect. Screeners should explore and document the assessment completed pursuant to Section 123605 of the Health and Safety Code, which identifies indicators of risk affecting the infant’s health and safety. -
Other high-risk birth (in-home only). No acts or omissions constituting neglect have yet occurred; however, conditions are present that suggest that the only reasons neglect has not occurred are the external supports of the hospitalization or the limited time since birth. Examples include but are not limited to the following:
- Sole caregiver or both caregivers have not attended to the newborn in the hospital.
- A caregiver with apparent physical, emotional, or cognitive limitations has no support system and may be unable or unwilling to meet the newborn’s basic needs.
- A child was born with medical complications, and sole caregiver’s or both caregivers’ response suggests caregiver(s) will be unable to meet the child’s exceptional needs (e.g., does not participate in medical education to learn necessary care, indicates denial of diagnosis, etc.).
Sexual Abuse
- Toddler or elementary school–aged child displays highly sexualized aggressive behaviors.
- Pre-adolescent child has initiated sexual acts or activities with caregivers, family members, or peers that are outside age-appropriate exploration or development, and this has led to a concern that they are a victim of sexual abuse.
- Child complains of pain in the genital or anal area AND there are other indications of sexual abuse.
Caregiver actively involved child/youth in acts of exploitation or trafficking. Caregiver involves the child in obscene acts or engages the child in prostitution or pornography. This includes a child being commercially sexually exploited and/or sex trafficked by or with knowledge and consent of caregiver. In this circumstance, an allegation of sexual abuse should be applied to the caregiver AND any third-party perpetrators.
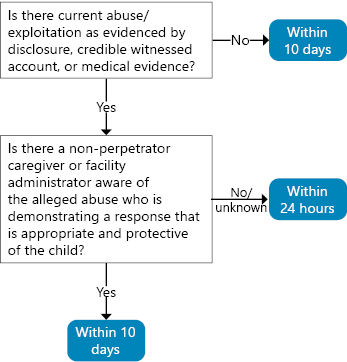
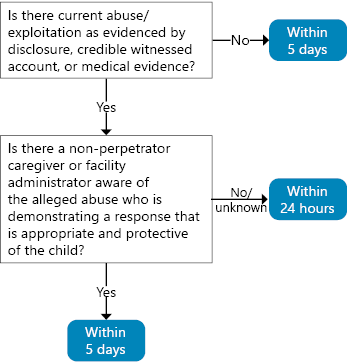
Child/youth is exploited or trafficked by someone other than a caregiver. Child/youth is being commercially sexually exploited by a person who is not a caregiver. Select if an in-person response is needed to assess the extent to which a caregiver has acted protectively OR has the ability to protect the child from exploitation. If this item is selected, an allegation of sexual abuse should be applied to only the alleged perpetrator(s) of the actual exploitation. Do not apply an allegation of sexual abuse to the caregiver.
Known or highly suspected sexual abuse perpetrator lives with child. An individual with a known or suspected criminal history of sexual crime, regardless of whether they have been arrested or convicted, lives in the same residence as the child.
Severely inappropriate sexual boundaries. Note: This does not include incidents that are accidental or inadvertent unless the report indicates that the behavior is persistent or frequently occurring.
- Adults in the home allow children to see sexually explicit material, witness sexual acts, or hear sexual language that is inappropriate to their age/developmental status; AND
- This has resulted in the child exhibiting age-inappropriate sexual behavior OR emotional distress.
- Adult(s) in the household exhibits behaviors suggesting the purpose is sexual gratification for the adult.
Consider whether a cross-report to another agency (Community Care Licensing, law enforcement or other county jurisdiction or agency) as required by state statute and regulations and local policy; if so, select the check-box. Make the cross-report immediately or as soon as possible to the appropriate jurisdiction according to state and local policy.
Note: While agreement with the decision is not required, attempts to reach consensus are considered best practice.
Document details about the collaborative assessment and the tribe’s position on the final screening decision in CWS/CMS.
Concern does not meet the criteria for in-person response, but it will be assigned based on MPP guidelines or local protocol. Select this override only after reviewing the appropriate SDM items and thresholds to confirm that an override is required.
As allowable by MPP 31-101.4, despite not meeting criteria for assignment, a concern about abuse, neglect, or exploitation will be assigned for response based on law enforcement request and local protocol.
A local protocol determines that a tribe may request a courtesy interview for in-person CWS response.
- Insufficient information to locate child/family. The caller was unable to provide enough information about the child’s identity and/or location to enable an in-person response. Select ONLY after following county protocol for attempting to discern identity/location from information provided by caller.
- Another community agency has jurisdiction, AND the report does not allege abuse or neglect in out-of-home care to a dependent or ward child/youth. Local protocol determines that an agency such as law enforcement, probation, or court will be the investigating entity for this issue AND a child welfare response is not required. Cross-report to law enforcement or the appropriate agency as required by state regulation.
- Historical information only. Child is at least 10 years old AND the alleged maltreatment occurred more than one year ago, AND there were no reports of abuse or neglect since the alleged incident, AND the conditions that contributed to the alleged incident are no longer present. If reported incident is sexual abuse, all of the above criteria must apply AND the reported perpetrator must be either an unidentifiable non-household member or deceased.
Physical Abuse
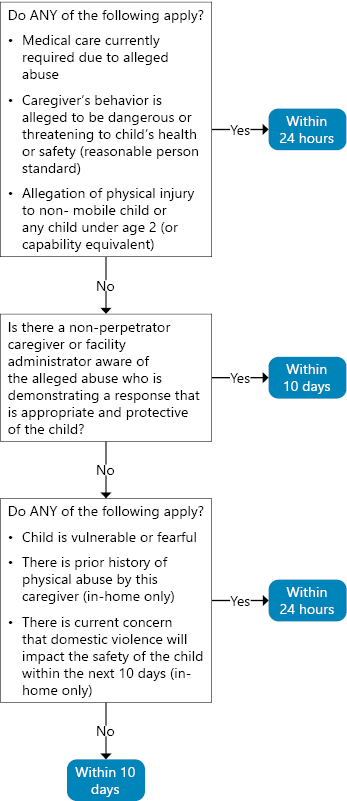
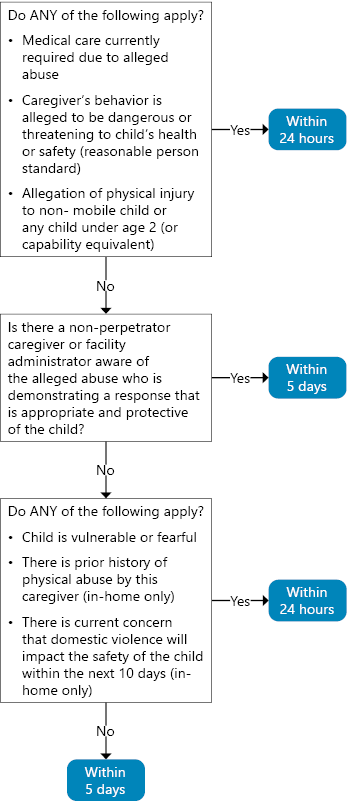
Caregiver acted in brutal or dangerous ways; or the caregiver has made threats (other than empty threats or threats made solely for intimidation) of brutal or dangerous acts toward the child AND absent intervention, it is likely that the child will experience an injury within the next 10 days.
Include concerns of caregiver substance use/abuse or current mental health issues that may increase the risk of physical injury or result in physical injury.
Examples include but are not limited to:- Hitting with closed fist;
- Hitting child's head, back, or abdomen with substantial force;
- Choking, kicking, or hitting with belt buckle or other dangerous object;
- Using restraints;
- Poisoning; or
-
Other actions that could reasonably result in severe injury, such as:
- Dangling the child from heights;
- Exposing the child to dangerous temperature extremes; or
- Throwing objects at the child that could cause severe injury.
- A child is vulnerable if, due to age, developmental status, or physical disability, they are unable to protect themself and/or will not be seen within the next week by other adults who would report concerns (e.g., school personnel).
- The child expresses credible fear of going/remaining home.
There is credible information that there are one or more prior investigations for physical abuse. (Include all investigations assigned for in-person response. If for a differential response county, include Path 2 and Path 3 referrals.)
Credible information includes statements by a reporter, verified information in CWS/CMS, or police reports.
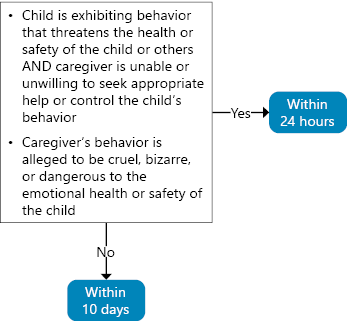
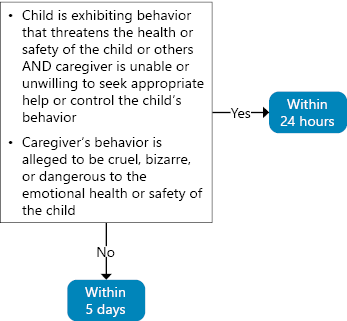
Emotional Abuse
- Attempted or threatened suicide.
- Cutting or other self-harmful behavior.
- Violent behavior toward others involving weapons.
- Threats of violence that involve weapons and there is reason to believe the child will carry out the threat.
- Violence toward very young or vulnerable children.
- Torturing or killing animals.
- Fire-setting behavior.
- The caregiver harms themself, others, or pets in the child’s presence.
- The caregiver threatens to harm themself, others, or the child’s pet.
- Unusual forms of discipline that rely on humiliation, fear, and intimidation, such as forcing a 10-year-old to wear diapers.
- Extreme rejection of the child, such as not speaking to the child for extended periods, acting as if the child is not present for long periods, or misusing time-out technique by using time limits far beyond what would be appropriate for the child’s age/developmental status.
- Domestic violence incidents that involve weapons or result in serious injury to any adult, or during which the child attempts to intervene or is directly in the path of violence.
Neglect
- Leaking gas from stove or heating unit.
- Substances or objects accessible to the child that may endanger their health and/or safety.
- Lack of water or utilities (e.g., heat, plumbing, electricity) and no alternative or safe provisions have been made.
- Open/broken/missing windows.
- Exposed electrical wires.
- Child has suffered serious illness or significant injury due to living conditions, and these conditions still exist (e.g., lead poisoning, rat bites).
- Guns and other weapons are not locked.
- Child is currently alone (time period varies with age and developmental stage).
- Caregiver does not attend to the child to the extent that need for care/protection goes unnoticed or unmet (e.g., child being harmed by another person in the home/failure to protect; the caregiver is present, but the child can wander outdoors alone, play with dangerous objects, play on unprotected window ledge, or be exposed to other serious hazards; a child with some suicidal ideation is not closely monitored).
- Child is presently receiving inadequate and/or inappropriate child care arrangements.
- Child has been abandoned and has no caregiver willing and able to provide care for a minimum of 10 days.
- Child/youth is being sexually exploited or trafficked, and information exists that the caregiver is unable or failing to provide supervision that would address immediate safety concerns within the next 10 days.
- The caregiver uses substances, such as methamphetamine, heroin, or cocaine, that typically result in severely impaired ability to function.
- The frequency and/or quantity of caregiver substance use suggests a high probability that they will be unable to meet the needs of the newborn upon discharge.
- Prior failed reunification.
Sexual Abuse
Policy
Law enforcement requests an immediate response. A law enforcement officer is requesting an immediate child protective services response.
Forensic considerations would be compromised by slower response. Physical evidence necessary for the investigation will be compromised if the investigation does not begin immediately, OR there is reason to believe statements will be altered if interviews do not begin immediately. There is reason to believe that the family may flee. The family has stated an intent to flee or is acting in ways that suggest an intent to flee, OR there is a history of the family fleeing to avoid investigation.Child safety requires a strategically slower response. The child's current location is such that initiating contact may create a threat to the child's safety OR the value of coordinating a multi-agency response outweighs the need for immediate response.
The child is in an alternative safe environment. The child is no longer in the same place or no longer with the caregiver who is the alleged perpetrator, and the child is not expected to return within the next 10 days (five days in Los Angeles).
The alleged incident occurred more than six months ago AND no maltreatment is alleged to have occurred in the intervening time period. The incident being reported occurred at least six months prior to the report AND no other maltreatment is alleged to have occurred in the intervening time period.
If reported concerns involve alleged harm to a dependent or dual-status child/youth in out-of-home care, the county where the facility is geographically located should respond to reports with a 24-hour response priority. Reports with a 10-day response priority should be referred to the placing county.
For all referrals that are evaluated out, select yes or no to indicate whether any of the following are applicable based on information reported or available at the time of the report. If unknown at the time of report, answer no.
- A caregiver has a substance abuse problem. The caregiver’s recurring use of alcohol or drugs causes functionally significant impairments, such as health problems, disability, or failure to meet responsibilities at work, school, or home.
- An adult household member exerts physical violence or patterns of power and control over another adult living in the home, impacting family functioning, regardless of whether children were present. This includes situations where one of the adults does not live in the home but has substantial contact in the home, or has lived in the home but continues to behave in threatening ways toward household members.
- A caregiver has current mental health concerns based on a diagnosis of a major mental illness (e.g., schizophrenia, bipolar disorder, depression) or exhibits symptoms that suggest a probability that such a diagnosis exists, such as hearing voices, paranoid thoughts, severe mood changes, suicidal thoughts or behavior, or extremely depressed affect.
- Mental health/behavioral problems. Problems unrelated to a physical or developmental disability (includes ADHD/ADD), which may be indicated by a Diagnostic and Statistical Manual of Mental Disorders (DSM) diagnosis, receipt of mental health treatment, attendance in a special classroom because of behavioral problems, or current psychoactive medication prescription.
- Developmental or physical disability. A severe, chronic impairment that creates substantial functional limitations in three or more of the following life activity areas: self-care, language, learning, mobility, self-direction, potential for independent living, and potential for economic self-sufficiency as an adult.
- Medically fragile or failure to thrive. A diagnosed medical condition that can become unstable and change abruptly, resulting in a life threatening situation (e.g., uncontrolled diabetes, required use of monitor, non-ambulatory child who requires 24-hour care, required nasal gastric or gastronomy tube, tracheotomy) or diagnosis of failure to thrive.
- Positive toxicology screen at birth. Positive screen for alcohol or another drug at birth.
- Delinquency history. Any child in the household has been referred to juvenile court for delinquent or status-offense behavior. Status offenses that have not been brought to court attention but have created stress within the household should also be scored, such as children who run away or are habitually truant.
- The family has housing, but the current housing situation is physically unsafe to the extent that it does not meet the health or safety needs of the child (e.g., exposed wiring, inoperable heat or plumbing, roach/rat infestations, human/animal waste on floors, rotting food).
- The family is homeless or was about to be evicted at the time the investigation began. Consider as homeless people who are living in a shelter and those living on a short-term basis with relatives or friends.
Specify whether this applies to the primary, secondary, or both caregivers.